
Pandemic preparedness means building stockpiles of food, medications, and PPE before an outbreak, establishing home monitoring and quarantine protocols, maintaining a 3–6 month emergency fund, and developing community support networks. Core supplies should cover at least 90 days. Pandemics typically last years, requiring sustained financial and physical resilience, not just short-term emergency measures.
Key Takeaways
- Stock a 90-day supply of medications, food, and PPE now — not during the next pandemic when shelves are already empty.
- A $25 pulse oximeter catches life-threatening respiratory decline before you feel short of breath — log readings daily alongside temperature.
- The 1918 St. Louis vs. Philadelphia comparison proves that acting weeks before it feels necessary saves the most lives.
- Your emergency fund is your most critical pandemic prep — 3 to 6 months of expenses protects you when the virus doesn't kill but unemployment might.
- Pandemics last years, not weeks — plan for sustained disruption including mental health, deferred medical care, financial resilience, and supply chain degradation.
Pandemic preparedness is the process of building household, community, and systemic resilience against infectious disease outbreaks through advance stockpiling, planning, skill development, and financial readiness. It’s not about predicting which virus comes next — it’s about making sure your family can sustain itself through months of disruption no matter what pathogen causes it.
Quick Summary
- Stock 90+ days of food, medications, PPE, and hygiene essentials before a pandemic — not during one when shelves are already bare.
- A pulse oximeter and digital thermometer are your most important home monitoring tools, catching dangerous declines before symptoms feel severe.
- History repeats itself: the 1918 Spanish Flu and COVID-19 both prove that early action — weeks before it feels necessary — saves the most lives.
- Financial resilience matters as much as physical supplies — build an emergency fund covering 3 to 6 months of essential expenses.
- Pandemics last years, not weeks — plan for sustained disruption including mental health, deferred medical care, and supply chain degradation.
- Community networks multiply your resilience — coordinated mutual aid reduces individual risk better than any solo stockpile.
The five core pillars of pandemic preparedness:
- Supplies — food, water, PPE, medications, and hygiene essentials for 90+ days
- Medical readiness — home monitoring tools, first aid skills, and medication reserves
- Financial buffer — 3 to 6 months of essential expenses in accessible savings
- Communication plan — family coordination, neighborhood networks, and information protocols
- Mental health — routines, entertainment, social connection strategies, and stress management
I’ve spent over 12 years in emergency management across the Pacific Northwest, including FEMA-certified training and hands-on work as a Wilderness First Responder. During the first COVID-19 wave in March 2020, I watched our local rural pharmacy run out of albuterol inhalers within 72 hours of the state emergency declaration. That moment crystallized something I’d been teaching for years: pandemic preparedness isn’t theoretical. It’s the difference between watching a crisis unfold on the news and living through one with your family protected.
This guide draws on the hard lessons of the 1918 Spanish Flu and COVID-19 to give you a pandemic preparedness plan that actually works.
What Caused the Spanish Flu and Where Did It Start
The 1918 pandemic was caused by an H1N1 influenza A virus — the same broad family of viruses that still circulates today. Where exactly it originated remains debated. The leading theory points to military camps in Kansas, specifically Camp Funston at Fort Riley, where a company cook named Albert Gitchell reported sick on March 4, 1918. Within weeks, over 500 soldiers at the camp were ill. Competing theories place the origin in France — where troops from multiple nations lived in crowded, unsanitary trenches — or in China, where laborers were recruited to support the Allied war effort.
So why “Spanish Flu” if it almost certainly didn’t start in Spain? Wartime censorship. The nations fighting World War I all suppressed press coverage of the outbreak to maintain morale. Spain was neutral, so its media reported freely on the devastating illness sweeping through Madrid. The world associated the disease with Spain simply because Spain was the only country honest enough to talk about it.
Understanding the origins matters for your pandemic preparedness plan because the same risk factors that spawned the 1918 outbreak still exist today. Zoonotic spillover — viruses jumping from animals to humans — remains the primary mechanism for novel pandemics. Crowded living conditions accelerate spread. And global travel means a virus that emerges on one continent reaches every other continent within weeks, not months. The next pandemic won’t start in a military camp in Kansas. It might start in a wet market, a factory farm, or a bat cave. But the pattern will be the same.
How Pandemics Spread: From Patient Zero to Global Crisis
Understanding how a disease outbreak spreads isn’t just academic — it directly determines your PPE choices, your ventilation strategy, and your isolation protocols. Both the 1918 flu and COVID-19 spread primarily through respiratory droplets and aerosols. When an infected person coughs, sneezes, talks, or even breathes, they release virus-laden particles into the air. Larger droplets fall to surfaces within a few feet. Smaller aerosol particles can hang in the air for minutes to hours in poorly ventilated spaces.
The concept of R0 (pronounced “R-naught”) describes how contagious a disease is in practical terms. For the 1918 flu, the R0 was estimated at 2 to 3. Early COVID-19 variants had a similar R0, but later variants like Omicron pushed that number above 10. In plain English: the higher the R0, the faster it moves through a population, and the harder it is to contain.
What does this mean for you at home? Crowded, poorly ventilated indoor spaces are where pandemics accelerate. In 1918, military barracks and troop transport ships were perfect incubators. In 2020, cruise ships, meat-packing plants, and dense urban apartment buildings served the same function. The physics haven’t changed.
Symptom Progression: Then vs. Now
Symptom progression differed between the two pandemics in ways that matter for home monitoring. The 1918 flu was notorious for sudden, violent onset — a soldier could feel fine at morning roll call and be dead by evening. The mechanism was a cytokine storm, where the victim’s own immune system overreacted so violently that it destroyed lung tissue. That’s why it disproportionately killed healthy young adults with robust immune systems. COVID-19 typically had a more gradual onset — fever, fatigue, dry cough — with a dangerous delayed phase around days 7 to 10 when some patients developed silent hypoxia and rapid deterioration.
Knowing what to watch for — sudden desaturation on a pulse oximeter, persistent fever above 103°F, confusion, or bluish discoloration around the lips — can mean the difference between seeking care in time and waiting too long.
The Historical Record: 1918 Through COVID-19
In the spring of 1918, H1N1 influenza began circulating in military camps across the United States. By the time it burned itself out in 1920, the Spanish Flu had infected an estimated 500 million people — roughly one-third of the world’s population — and killed between 50 and 100 million, including 675,000 Americans.
Here’s the part most people miss. The first wave in spring 1918 was relatively mild. People relaxed. Cities lifted restrictions. Then the second wave hit in the fall, and it was catastrophically deadlier. A significant factor in the enormous death toll was secondary bacterial pneumonia — in an era before antibiotics, patients who survived the initial viral assault often succumbed to bacterial infections in their damaged lungs. Had antibiotics existed in 1918, millions of lives could have been saved.
Philadelphia held a parade. St. Louis canceled gatherings. Six weeks later, Philadelphia had buried 12,000 people — and St. Louis’s death rate was less than half.
Philadelphia held a massive parade on September 28, 1918, despite warnings. Within 72 hours, every bed in the city’s 31 hospitals was full. Within six weeks, 12,000 Philadelphians were dead. St. Louis, which canceled public gatherings early and enforced strict quarantine measures, saw a death rate less than half of Philadelphia’s. The lesson? Timing isn’t everything — it’s the only thing.
Fast forward a century. When COVID-19 emerged from Wuhan, China in late 2019, most of the world watched the news for weeks before it arrived at their doorstep. We had warning. And yet, by the time the WHO declared a pandemic on March 11, 2020, the virus was already spreading silently across Europe and North America. The official global death toll surpassed 7 million, though excess mortality studies suggest the true number is significantly higher.
But COVID didn’t just kill through infection. It exposed the staggering fragility of modern supply chains — remember when you couldn’t buy toilet paper, hand sanitizer, or a simple box of N95 masks? It showed that hospitals could be overwhelmed not by a single catastrophic event but by a slow, relentless wave. And it demonstrated that job loss, isolation, deferred medical care, and mental health collapse are as much a part of a pandemic as the virus itself.
Between these bookend events, we’ve had SARS in 2002-2003 (8,098 confirmed cases, 774 deaths), which proved aggressive quarantine and contact tracing can contain a respiratory virus. MERS in 2012 showed that zoonotic spillover from camels could create another coronavirus threat. And the Ebola outbreak of 2014-2016 killed more than 11,000 people across West Africa, proving the life-or-death importance of contact tracing and proper PPE protocols. Each of these events was a dress rehearsal. Each time, the world largely forgot the lessons within a few years.
How Did the Spanish Flu End — And What That Tells Us
One of the most common questions I hear is “how long did the Spanish flu last?” Roughly two years, from early 1918 through spring 1920, with three distinct waves. But understanding how it ended matters more than the timeline.
The 1918 pandemic ended through a combination of three factors — none of which was a vaccine. First, natural immunity built up across surviving populations. After two years of waves, enough people had been infected and recovered that the virus had fewer susceptible hosts. Second, the virus mutated toward less lethal strains. This is a common evolutionary pattern — viruses that kill their hosts quickly are less efficient at spreading than those that cause milder illness. Third, improved public health measures reduced transmission enough to let the pandemic burn down.
Here’s the critical takeaway: “ending” doesn’t mean “disappearing.” The H1N1 virus that caused the 1918 pandemic didn’t vanish. Its descendants continued to circulate for decades and were responsible for another pandemic in 2009 (the H1N1 “swine flu”). COVID-19 followed a similar trajectory — vaccines accelerated the transition from pandemic to endemic phase, but the virus didn’t go away.
For your pandemic preparedness plan, this means planning for an endemic phase is just as important as planning for the acute emergency. Ongoing boosters, updated stockpiles, periodic reassessment of your supplies, and the financial resilience to absorb years of economic disruption aren’t optional add-ons — they’re the core of long-term disease outbreak preparedness.
How Much Warning You’ll Actually Get
Here’s the honest truth about pandemic warning time: you’ll probably have weeks to months of news coverage about a disease spreading in another country before it shows up locally. That’s a luxury almost no other disaster affords you. An earthquake gives you zero seconds. A tornado gives you minutes. A pandemic gives you a window that most people waste arguing about whether it’s “really that bad.”
The signals are predictable: unusual disease clusters reported by the WHO, travel advisories, country-level lockdowns overseas, and eventually your own government issuing cautious statements that somehow manage to simultaneously downplay and alarm. COVID followed this exact playbook. We watched Wuhan lock down in January 2020. Italy’s hospitals collapsed in early March. Americans had roughly six to eight weeks of visible, escalating warning — and most people used that time to do absolutely nothing.
Once community transmission begins locally, your window shrinks to days, not weeks. Shelves start emptying fast. The items that disappear first aren’t the ones you’d expect — they’re psychological comfort items (toilet paper, cleaning supplies) followed quickly by the genuinely critical ones (medications, masks, shelf-stable food). Urban residents feel the squeeze faster because supply chains serve dense populations on a just-in-time basis, meaning stores carry only about three days’ worth of inventory at any given time. Rural residents have slightly more buffer but fewer nearby options when things run out.
The time to prepare is when the news feels distant and theoretical. If you’re buying supplies the same week your governor declares a state of emergency, you’re already competing with millions of people who had the same late realization.
The First 72 Hours of a Pandemic Emergency
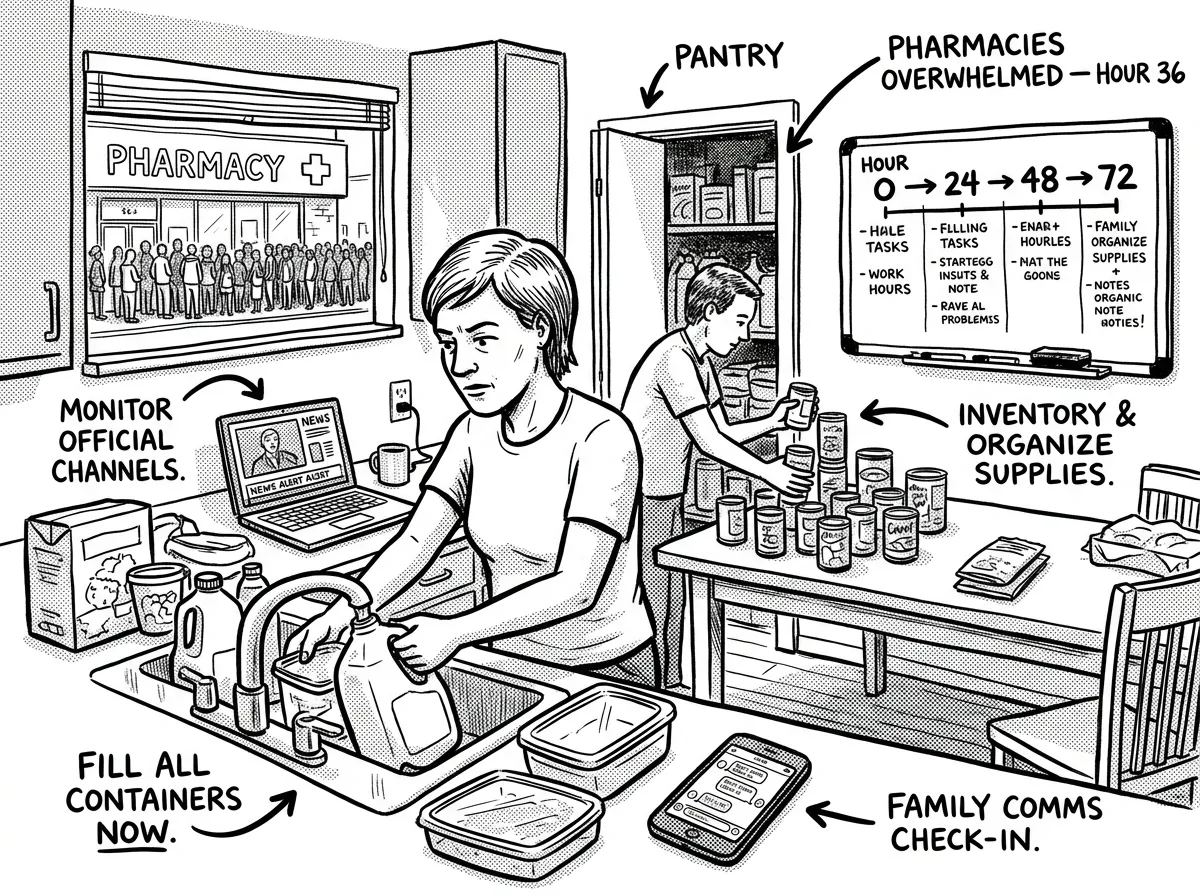 Critical actions in the first three days after a pandemic declaration
Critical actions in the first three days after a pandemic declarationThe first 72 hours of a locally declared pandemic emergency feel less like a disaster movie and more like a slow, creeping anxiety attack. No explosion. No sirens. Your phone buzzes with a news alert. Schools announce closures. Your employer sends a vague email about “monitoring the situation.” Then you walk into a grocery store and see the empty shelves, and something in your chest tightens because you realize this is actually happening.
In the first hour, your job is simple: don’t panic-shop. If you’ve been following a pandemic preparedness plan, you already have what you need at home. If you haven’t, your priority list is ruthlessly short — prescription medications, shelf-stable food, fever reducers, and hygiene supplies. Get them calmly and get home. If you need a quick framework, building a 72-hour emergency kit covers the absolute essentials for any emergency’s opening days.
In the first 24 hours, the immediate threat isn’t the virus — it’s the breakdown of routine. You need to establish your household’s operating protocol. Who’s going out and who’s staying in? What are your hygiene procedures for items entering the house? Do you have a way to monitor symptoms?
A digital thermometer and a pulse oximeter — around $25 combined — become two of the most important tools in your home. I personally used pulse oximetry to monitor my household when two family members came down with COVID in January 2022. Watching one of them drop from 96% to 91% SpO2 over six hours told me it was time to call the doctor — before anyone felt especially short of breath. That device paid for itself a thousand times over.
Setting Up a Home Quarantine Room
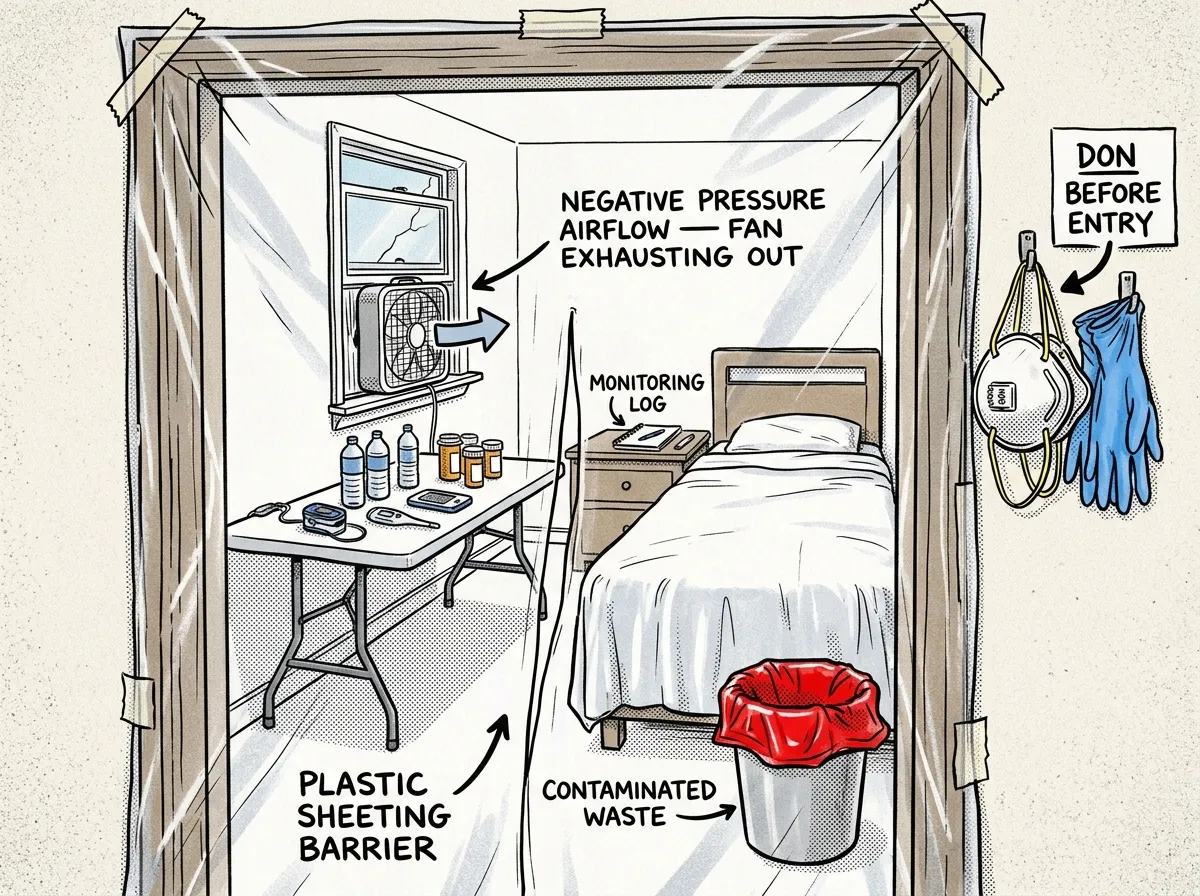 Designating and equipping an isolated quarantine space in your home
Designating and equipping an isolated quarantine space in your homeSet up a quarantine room in your home in case a household member gets sick. Choose a room with a door that closes and ideally its own bathroom. If you only have one bathroom, the sick person uses it last, then surfaces get wiped down with disinfectant.
- Water bottles (enough for 3+ days)
- Thermometer and pulse oximeter
- OTC medications (fever reducers, electrolytes)
- Tissues and lined trash can with lid
- Disinfectant wipes or spray
- Phone charger
- Clean towels
- Notebook for symptom logging
Tape a towel along the bottom of the door gap to reduce airflow to the rest of the house. Open the room’s window slightly for ventilation if weather allows. It’s not a hospital isolation unit, but in my experience, this basic setup dramatically reduces household transmission.
By hour 48 to 72, the reality of isolation starts setting in. If your area is under stay-at-home orders, you’ll notice how quickly boredom, anxiety, and cabin fever emerge — especially in households with children. This isn’t trivial. During COVID, domestic violence calls surged by 25-33% globally, mental health crises skyrocketed, and substance abuse spiked dramatically. The first 72 hours is when you set the psychological tone for what could be weeks or months of disruption. Establish routines. Assign responsibilities. Limit news consumption to specific check-in times rather than a constant drip of anxiety. If you’ve built your preparedness foundation ahead of time — and if you’re new to this, our beginner’s guide to survival readiness is a solid starting point — the first 72 hours should feel manageable, not desperate.
When Days Become Weeks
After the initial shock wears off, a pandemic settles into a grim rhythm. The systems that break down follow a predictable order.
Healthcare goes first. Hospitals fill, then overflow. Elective surgeries get canceled — and “elective” includes biopsies, joint replacements that let people walk, and diagnostic procedures that catch cancer early. During COVID, ER wait times in some U.S. cities stretched to 12+ hours, and ambulance response times doubled or tripled.
Supply chains degrade next. Not a dramatic collapse, but a death by a thousand cuts — certain medications become scarce, specific food items vanish, shipping times extend from days to weeks.
Then economic disruption hits. Businesses that can’t operate remotely start laying off workers. During COVID, the U.S. unemployment rate hit 14.7% in April 2020 — the highest since the Great Depression. If you don’t have a pandemic emergency fund, you’re dealing with a health crisis and a financial crisis simultaneously.
Weeks two through six are where the real grind begins. Your 3-month food supply starts looking less like paranoid overkill and more like basic common sense. This is also when secondary health threats spike — people skip dialysis appointments, delay chemotherapy, or ignore chest pain because they’re afraid of the hospital. During COVID’s first year, excess deaths from heart disease, diabetes, and other chronic conditions increased significantly beyond what the virus itself caused. Your ability to manage routine health at home — monitoring vitals, maintaining medication schedules, treating minor ailments without a doctor visit — becomes a genuine survival skill.
Long-Term Disruption: When It Doesn’t Resolve Quickly
The Spanish Flu lasted roughly two years with multiple waves. COVID-19’s acute emergency phase stretched from early 2020 well into 2022 in most countries. If you’re hoping the next pandemic wraps up in a few weeks, history isn’t on your side.
Daily life transforms in ways that go far beyond wearing a mask to the grocery store. Remote work becomes the assumed norm. Education shifts online, often poorly. Social isolation becomes chronic, and its effects compound: depression, anxiety, loss of community, radicalization through excessive online engagement. Children who spent formative years in isolation showed measurable learning loss and social development delays that educators are still trying to address years later.
New threats emerge that aren’t obvious at the outset. Supply chain adaptation means certain goods become permanently more expensive or scarce. Inflation spikes — the post-COVID inflation surge was driven partly by pandemic-era supply disruptions and stimulus spending. Political polarization intensifies. Trust in institutions erodes, which makes the next pandemic even harder to manage because public compliance with health measures depends on trust.
Perhaps most critically, your financial resilience becomes the single biggest predictor of how well you weather a prolonged pandemic. The virus may not discriminate, but its economic consequences absolutely do. An emergency fund covering 3-6 months of expenses isn’t aspirational advice — it’s the difference between riding out a disruption and losing your home. If you’re starting from scratch, our guide to building an emergency fund for preppers walks through the process step by step. A solid foundation in overall preparedness, including practical self-reliance skills, gives you options and confidence when the systems you’ve relied on become unreliable.
Your Pandemic Preparedness Checklist
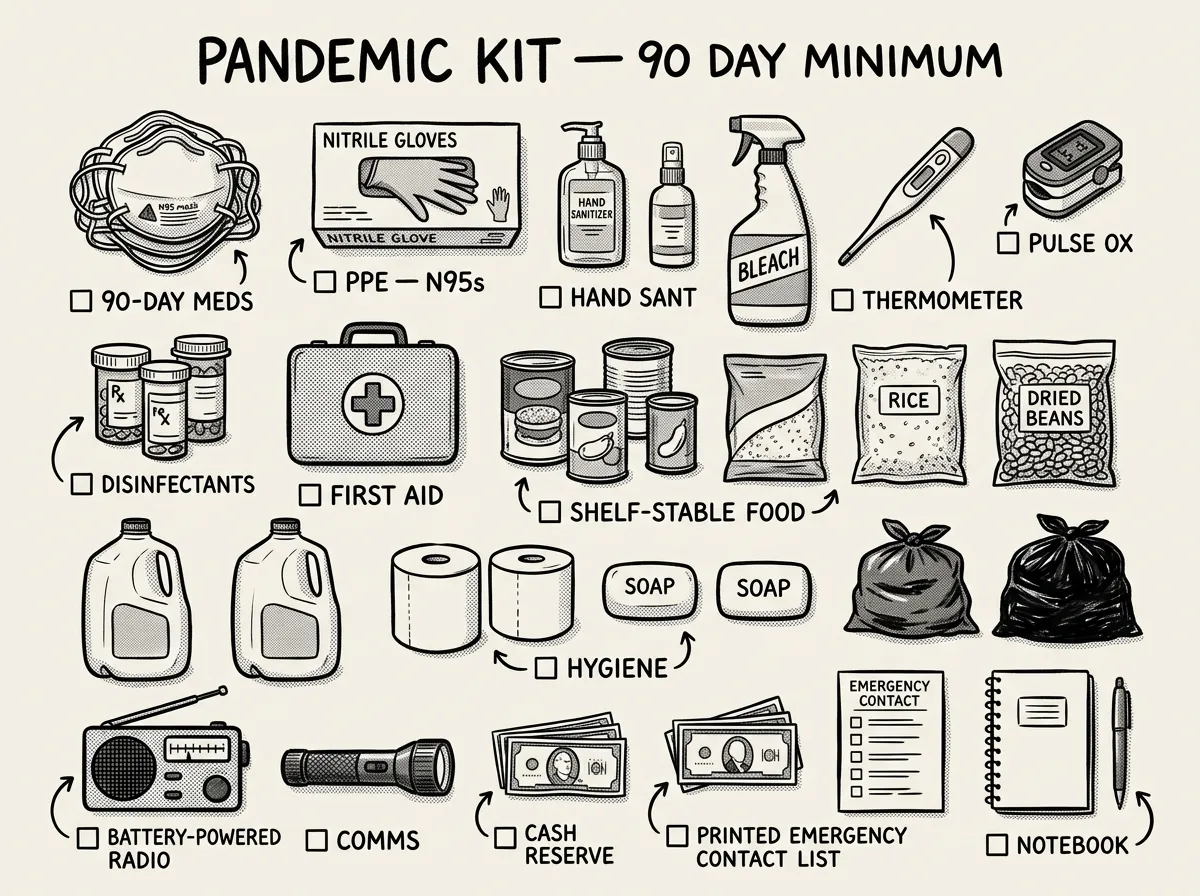 Complete pandemic preparedness kit spread for inspection
Complete pandemic preparedness kit spread for inspectionI’ve broken this pandemic supply list into three phases and three budget tiers so you can start where you are and build over time.
Phase 1: Before — Building Your Foundation (Do This Now)
Tier 1 — Under $100, do this week:
- Pulse oximeter — one per household. A reliable fingertip model costs around $20-$30. Normal SpO2 is 95-100%. Below 92% warrants medical attention.
- Digital thermometer — one primary and one backup. Budget around $15-$20 total.
- Hand sanitizer (at least 60% alcohol) — minimum 2 bottles, staged at your main entry point and vehicle. About $10.
- OTC medication starter stockpile: acetaminophen, ibuprofen, anti-diarrheal medication, electrolyte packets (Pedialyte or generic), and antihistamines. About $30-$40 total.
- Copies of critical documents — insurance cards, prescription lists, identification, financial account info — stored physically and in encrypted digital backup. Cost: just your time.
Tier 2 — Under $500, do this month:
- 90-day supply of prescription medications. Talk to your doctor about getting a 90-day supply instead of 30-day refills. Many insurance plans allow this through mail-order pharmacies. For controlled substances, start filling prescriptions a few days early each cycle to build a buffer.
- N95 or P100 respirators — minimum 20 N95s per household member. Not surgical masks, not cloth masks. Buy NIOSH-certified N95s — the 3M Aura 9205+ (around $25-$50 for a box of 20) is what I reach for every time. They’re widely available, comfortable for extended wear, and they actually seal. Whatever you buy, learn how to fit-test them at home — a mask that doesn’t seal is just decoration.
- Nitrile gloves in bulk — 2 boxes of 100. A few dollars per box when there isn’t a pandemic. During one, they become gold.
- Expanded OTC medication stockpile: add decongestants (pseudoephedrine — behind the pharmacy counter but no prescription needed), cough suppressants, and extra electrolyte packets. If your doctor will prescribe antivirals like oseltamivir (Tamiflu) in advance, ask. About $30-$50 additional.
- 3-month food supply requiring no shopping. Rice, beans, canned goods, pasta, peanut butter, oats, cooking oil, salt, honey, powdered milk, canned proteins, and multivitamins. Rotate stock using first-in, first-out. Budget roughly $200-$300 for a family of four. Our long-term food storage guide covers exactly what to buy and how to rotate it.
- Water preparedness — 1 gallon per person per day for a minimum of 14 days. For a family of four, that’s 56 gallons. Municipal water systems are unlikely to fail completely, but workforce shortages can degrade water treatment reliability. Our guide on emergency water storage and purification covers this in detail. Budget $30-$50 for storage containers and a gravity filter.
- Backup thermometer — add a battery or analog model. Batteries die at the worst times. $10-$15.
Tier 3 — Ongoing investment:
- Emergency fund covering 3-6 months of essential expenses. If you’re starting from zero, begin with a target of $1,000, then build. Automate transfers. Non-negotiable.
- Remote work capability. Reliable internet, a laptop, access to necessary software or VPN. If your job can’t be done remotely, your emergency fund needs to be larger.
- Entertainment and mental health supplies. Books, board games, art supplies, exercise equipment. Sounds trivial until you’re on week six of quarantine and your household is one argument away from a meltdown.
- Skill development — first aid certification, food preservation, basic home medical care. The first aid skills every prepper needs is a practical starting point that translates directly to pandemic scenarios.
Estimated total for Tier 1 + Tier 2 combined: $400-$600 for a family of four. That’s the cost of a single ER copay in most insurance plans — and it buys you 90 days of self-sufficiency.
Phase 2: During — Immediate Response
- Activate your hygiene protocol — designate a decontamination area at your home entrance for shoes, hand sanitizing, and clothes changes after high-exposure trips
- Establish your household quarantine room if a member becomes ill, stocked with water, medications, monitoring tools, and disinfectant
- Monitor symptoms daily — temperature checks and pulse oximetry for all household members every morning, logged in a notebook (trends matter more than single readings)
- Limit trips outside to essential needs only, batch errands, and maintain hygiene protocols for delivered packages during peak transmission
- Communicate with your support network — check in with elderly relatives, immunocompromised friends, and neighbors who live alone
- Ration wisely — calculate food supply against people and days, eat perishables first, then frozen goods, then shelf-stable supplies
Phase 3: After — Recovery and Reassessment
- Replenish everything you used. Restock medications, food, PPE, and financial reserves immediately while supplies are available and prices normalize. The next wave won’t wait for you to be ready.
- Document what worked and what didn’t. Which supplies did you burn through fastest? What did you wish you had? Where did your plan fail? I do this after every field deployment, and it’s the single most effective way to improve your preparedness.
- Address deferred medical care. Schedule those appointments you postponed. Get the screenings, dental work, and checkups that fell through the cracks. Secondary health impacts from delayed care are a leading cause of post-pandemic excess mortality.
- Rebuild your emergency fund if you drew it down. Priority one before any discretionary spending.
- Check expiration dates. Medications, food, and even hand sanitizer expire. Build a calendar reminder system to rotate stock quarterly.
Community Mutual Aid and Neighborhood Networks
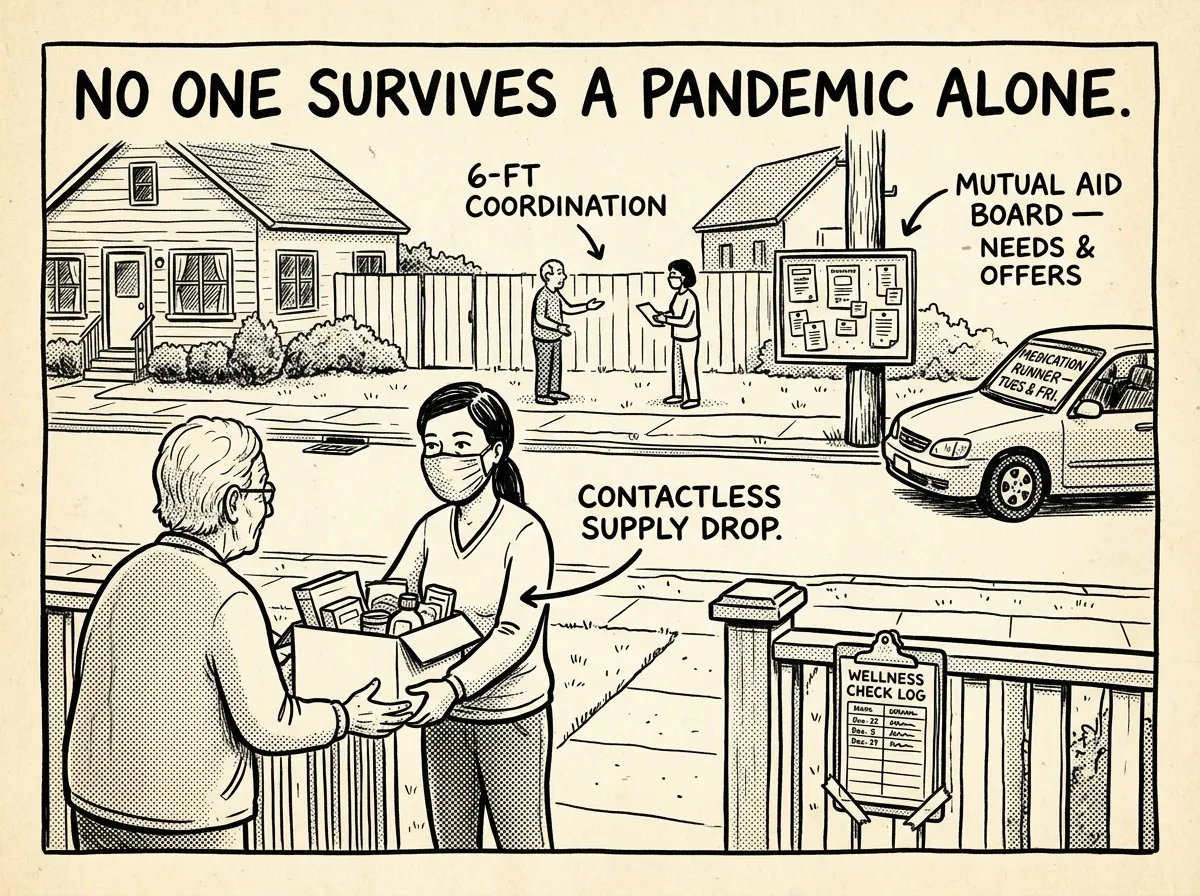 Neighbors coordinating supply sharing and wellness checks during extended lockdown
Neighbors coordinating supply sharing and wellness checks during extended lockdownHere’s something almost every pandemic guide gets wrong: they focus entirely on the household and ignore the community.
In my experience, the families that weathered COVID best weren’t the ones with the biggest stockpiles — they were the ones embedded in networks of mutual support. During the COVID winter of 2020-2021, a daily check-in call I made to an elderly neighbor revealed he’d run out of his blood pressure medication three days earlier and hadn’t told anyone. We had it resolved within hours. Without that call, the outcome could’ve been very different.
During both 1918 and COVID-19, organized community response saved lives that individual preparedness alone couldn’t. In 1918, volunteer organizations coordinated food delivery to quarantined households when no government agency had the capacity. During COVID, mutual aid groups sprang up across the country, delivering groceries to immunocompromised neighbors, organizing childcare for essential workers, and pooling resources to cover rent for laid-off community members.
How do you build this before a crisis?
Identify vulnerable neighbors. Walk your block. Who’s elderly and lives alone? Who’s immunocompromised? Who has young children and no nearby family? Knowing who they are before a crisis is half the battle.
Establish communication channels. Create a neighborhood group text, email list, or phone tree. If cell networks degrade under load (which happened in some areas during COVID), walkie-talkie radios on a shared channel provide backup. I keep a set of FRS radios charged and ready specifically for this purpose.
Coordinate supply runs. One person making a grocery run for four households means three fewer people exposed. During COVID, I organized rotating supply runs in our neighborhood — one person per week handled shopping for five families using a shared list. Total exposure reduced by 80%.
Share skills. Maybe you’ve got first aid training. Maybe your neighbor is a nurse. Maybe someone else has a generator or knows how to can food. Document these skills in a shared list so everyone knows who to call for what.
Isolation doesn’t mean going it alone. Coordinated community action reduces individual risk — that’s not idealism, it’s math.
What Most People Get Wrong
The single biggest mistake in pandemic preparedness is confusing information with action. During COVID, millions of people obsessively refreshed case count dashboards, argued about mask efficacy on social media, and watched hours of news coverage — while their pantries held three days of food and their medicine cabinets held a half-empty bottle of expired Tylenol. Knowing the R-naught of a virus doesn’t help you if you can’t feed your family for a month without going to a store.
I’ve watched people make this mistake over and over. They spend hours researching which variant is circulating and zero hours checking whether their prescriptions are stocked for more than a week. Information feels productive. It isn’t — unless it drives specific action.
The second biggest mistake is preparing for the wrong pandemic. People imagine a Hollywood-style plague — bodies in the streets, total civilizational collapse — and either over-prepare for an apocalypse that doesn’t come or dismiss preparedness entirely because it “wasn’t that bad.” Most pandemics look like COVID: a grinding, slow-burn disruption where the grocery stores are still open but half the shelves are empty, where hospitals still function but are rationing care, where life goes on but worse in a hundred small ways for months or years.
Your pandemic preparedness plan needs to match that reality — not a zombie movie. Build for the grind. Build for the long disruption. Build for the world where you can’t get your kid’s medication refilled for three weeks and the ER has a 14-hour wait. That’s the pandemic most of us will actually face. And it’s the one you can absolutely prepare for — starting today.
The Complete
Prepper's Reference.
149 articles synthesized into one comprehensive PDF — twelve chapters covering water, food, shelter, first aid, comms, and scenario-specific preparedness. Free with your email.
Unsubscribe anytime · We never share your email
You're in. Check your inbox.
Keep Reading
Volcanic Eruption Preparedness: When the Mountain Wakes Up
Mount St. Helens gave scientists 2 months of warning — yet 57 people still died. The 2022 Tonga eruption sent a shockwave around the planet twice. Here's what volcanic eruptions actually threaten, how far danger extends, and how to prepare whether you live near a volcano or not.
Cyberattack and Infrastructure Failure: The Invisible Emergency
In 2021, a ransomware attack shut down the Colonial Pipeline and caused gas shortages across the Southeast in 6 days. In 2015, hackers turned off power for 230,000 Ukrainians. Digital attacks on physical infrastructure are here — here's how to prepare for when they hit yours.

Tsunami Preparedness: What to Do When the Ocean Retreats
The 2004 Indian Ocean tsunami killed 227,000 people in 14 countries in under 8 hours. A 10-year-old girl's geography lesson saved 100 lives on a Thai beach. Here's what tsunamis actually look like — and the knowledge that makes the difference between life and death.